

**Caution: Extended Coverage Of Cholesterol Ahead**
Cholesterol: such an amazing component of the human body yet maybe the most maligned substance in the world of health. I have written much on cholesterol in the past and am endlessly fascinated with everything about it. Just last week I shared a video from the Dr. Oz show where he took a step in the right direction on the topic of cholesterol. In writing that synopsis I realized how much info I have piled up to share on the topic so here we are… a giant post on cholesterol.
This mammoth will have three parts to it: the basics of cholesterol/blood lipids/testing, synopses of reviews on cholesterol by some leading researchers, and my collection of thoughts on where we need to keep looking for future cholesterol exploration.
Part 1: Review
The goal of this section is to get down to the basics of cholesterol. What is it, what does it do, how does your body transport it and what do the cholesterol blood tests mean? Some basics followed by an extensive, in-depth breakdown. Hopefully at the end you will have a much better understanding of the function of cholesterol in the human body.
Cholesterol: What is it?
A waxy steroid of fat produced by all cells in the body (including higher level production in the liver, intestines, adrenal and reproductive organs). Cholesterol is essential to life in mammals and is used in every cell of the human body. It is a fat soluble substance, meaning it is not transported freely in the water based blood, it needs to be carried by protein wrapped vesicles. Cholesterol is the cargo being transported inside ships/submarines (HDL, LDL, VLDL, etc.) that float through the blood.
Cholesterol: What does it do?
Cholesterol has several functions in the body, including…
1. It compromises cell membranes, giving them the proper permeability and fluidity.
2. It functions within the cell membrane in intracellular transport, cell signaling and nerve conduction.
3. It serves as the base for bile production, enabling proper digestion of fats.
4. It is the precursor to adrenal and sex hormones (cortisol, DHEA, testosterone, estrogen).
5. It leads to a derivative which converts sunlight into vitamin D.
6. It is also considered an antioxidant and is vital to the immune system.
7. It has functions and purposes we have yet to discover.
Cholesterol: How do your cells get it?
Nearly every cell in your body makes its own cholesterol but for cells in need of more, your body has a very savvy way of delivering the precious cargo through the blood stream via cargo ships called lipoproteins.
What are lipoproteins?
A family of five molecules – chlyomicrons, VLDL, IDL, LDL, HDL- (ranging in size from largest to smallest) that are responsible for transporting cholesterol, fatty acids and fat soluble vitamins in the water based blood stream. Every cell in our body needs these lipoproteins to function well and deliver its valuable cargo.
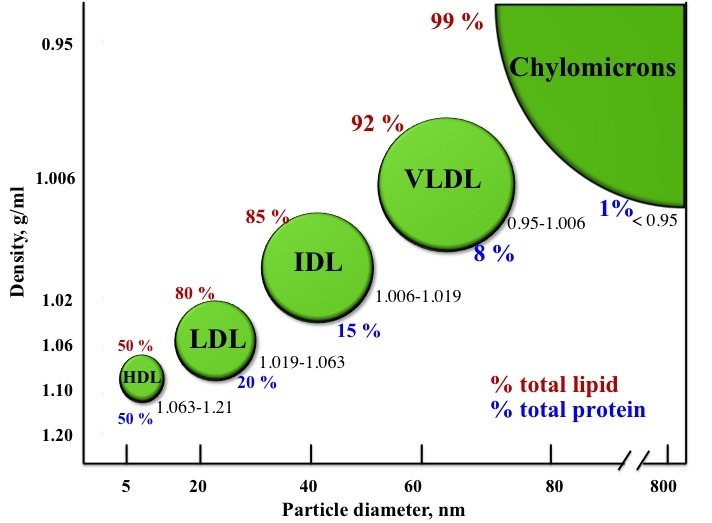
Courtesy of InTechOpen
The three largest, chylomicrons, VLDL (Very Low Density Lipoprotein) and IDL (Intermediate Density) all play important roles but are typically not addressed in routine lab work. VLDL, however, should be considered a valuable tool because it gives us great insight and clues to the status of many metabolic processes going on in the body (check out more on the function of VLDL in the expert review section). This review will focus on LDL and HDL, the two molecules most people are concerned with and the two that need the most explaining.
Common Thoughts/Beliefs:
1. LDL is bad because it puts cholesterol in your arteries and HDL is good because it cleans up cholesterol and takes it away from the blood vessels.
2. Small dense LDLs get stuck in cracks in the artery wall, large fluffy LDLs don’t.
**Spoiler alert: these are wrong.**
Here’s a lipoprotein molecule:
.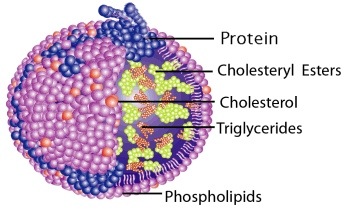
As you can see, the cargo (cholesterol, triglycerides, vitamins) are enclosed by a lipid and protein exterior. This is how cholesterol is transported, it does not float freely in your blood.
LDL
Low density lipoproteins, like all other lipoproteins, are molecules that transport nutrients to cells in the body. They are considered low density due to the lower ratio of protein to cholesterol than HDL, the highest and most dense lipoprotein. They start off as VLDLs, come in many different sizes and are a vital part of healthy function. Primarily, LDL particles carry cholesterol, fatty acids (triglycerides) and fat soluble vitamins and nutrients. They are the literal delivery trucks of substrate in the body. One of the main substrates they deliver is cholesterol, which is needed throughout the body for its numerous uses. However, because one of those deliveries can be to blood vessels to repair damage in the endothelial wall, LDL and its cholesterol gets a lot of criticism. Arterial plaque is made from cholesterol, protein and calcium yet somehow cholesterol is blamed for heart disease while protein and calcium continue to be two of the most heralded nutritional components around.
LDL particles carry the same cholesterol as HDL, yet have been termed bad due to the above behavior and correlation based research that shows higher LDL levels are associated with greater risk of cardiovascular disease. Once again, we are making life saving/risking decisions based off correlation without asking why the relationship exists or why might the body be carrying high levels of cholesterol in its LDLs. As a result, trying to simply intervene by limiting/lowering LDL cholesterol means limiting the amount of cholesterol LDL can transport to the body to use for normal functioning. Is it good to limit a substance the body has raised (probably for a reason)?
When the LDL particles spend too long in the blood stream or get stuck in the artery walls they can oxidize and present a problem. The solution doesn’t begin by blaming the cholesterol or even with the LDL, it lies in pursuing this question: WHY did the LDL get oxidized or stuck or spend too much time floating around? Why is it not getting used? Where is the oxidation coming from? Dealing with the cause of oxidation or cracks in the arterial wall is the issue. Not the LDL or the cholesterol. Innocent bystanders accused of a crime they simply witnessed.
HDL
High density lipoproteins are the theoretical heart saviors these days. A cholesterol transporter, HDLs are the smallest and densest lipoproteins with the greatest protein to cholesterol ratio. Most of their function is to collect cholesterol from other lipoproteins or body cells and deliver it to the liver or steroid glands for hormone production (e.g. adrenals, ovaries, testes). HDL acts as a “recycler” of cholesterol. It gives its cholesterol to VLDLs and LDLs to be delivered throughout the body (in exchange for triglycerides) and then continues its scouring journey.
The recycling function of HDL is the primary reason for their reputation. On the surface it seems like a fantastic molecule, picking up and recycling the cholesterol trash. That must be why high HDL cholesterol levels are good, right? Upon further examination, we know that the body is much more complex and there is no rogue trash cholesterol just floating around in need of picking up and therefore no such thing as good and bad cholesterol or lipoproteins, no matter how much our human brains want to assign blame and heroism.
HDL is associated with decreased levels of heart disease. Here’s the problem: correlation does not equal causation. HDL cholesterol raises with activity, particularly intense exercise which begs the question: is raising HDL levels protective or do healthy behaviors raise HDL levels? The more we understand the dynamics of cholesterol the more we can figure out why so many of these things happen in the body.
There are many versions of both LDL and HDL and this is important to a certain degree but for most of us, simply knowing the basics is good enough.
Cholesterol: What do cholesterol/blood lipid tests mean?
Typically blood lipid tests measure total cholesterol, LDL cholesterol, HDL cholesterol and triglycerides. The results of these tests are often misconstrued or misinterpreted, as it vitally important to understand what is actually being measured and what’s not. For the best picture, think of the ship/cargo analogy eluded to earlier. Picture this: In a small section of the river, the lab diverts the different ships (HDL, LDL, VLDL, etc.) to the dock, separates them, and then counts the cargo (cholesterol, triglycerides) in each group of ships for a sum in each subcategory and then adds it all up for a grand total. When you see a total cholesterol value, this is the total number of cholesterol molecules being carried by all lipoprotein particles in the sample of blood taken. Or: of all the ships sequestered regardless of type, what their total cargo adds up to. Whether it is 5 ships or 50 ships, comprised of any ratio of HDL, LDL etc., what is measured is how much cargo gets delivered. Five lipoprotein ships delivering 200 units of cholesterol will have the exact same “cholesterol score” as 50 delivering 200 units of cholesterol. As we will get to later, this distinction may be a very big deal and is one reason your total cholesterol score tells you very little. Remember, your cholesterol score does not tell you the number of HDL/LDL particles (ships) in your blood and not the amount of free floating cholesterol in your blood (which doesn’t happen). The lab also will do a separate analysis of how much cholesterol was in the HDL particles (your HDL cholesterol) and a LDL cholesterol count (your LDL cholesterol). So a LDL test result of 150 means you were measured to have 150 cholesterol molecules in the sample of LDL particles. Here is another catch: often your LDL cholesterol is calculated, meaning they don’t even count it, they estimate it based on other cholesterol counts. The number of ships in the blood likely matters much more than how much they carry (more details on this in the expert review section).
Here is the biggest point- what your doctor likely measures (cholesterol levels in your lipoproteins in the blood) has nothing to do with cholesterol in your arteries. Blood tests that report levels of cargo being carried tells us simply that: how much cholesterol your body is delivering through the blood at a given time.
The take away- cholesterol levels do matter in that they can be helpful in getting some insight into the body’s metabolic functioning. High, low or radically changing levels of cholesterol or lipoprotein particle counts tell us how the body is metabolizing and trafficking energy and substrates, along with hints into thyroid function and metabolic health and efficiency.
Most importantly, cholesterol and lipoprotein levels are clues into the body’s adaptive processes in response to the environment and stimuli you are exposing it to. Use this info to see how your body is responding to your lifestyle.
Part 2: What The Experts Are Saying
Since I like to keep up to date on the latest and greatest with cholesterol, let’s take a look at how 3 of the leading cholesterol authorities, Peter Attia, Chris Masterjohn and Thomas Dayspring, cover the issue, followed by a link to Ray Peat’s thoughts on cholesterol…
Dr. Peter Attia covers the cholesterol basics and a whole lot more
The Straight Dope on Cholesterol- 10 Things You Need To Know part 1 and part 2 as summarized by Marks Daily Apple. See more from Dr. Attia at The Eating Academy.
Here’s the 10 point synopsis:
1. Sterols (cholesterol) that end up in the artery wall is the problem but how they get there is what we need to worry about.
2. Cholesterol is vital for life; no cholesterol = no life.
3. The cholesterol we eat has little to do with the cholesterol we measure in our bloodstream.
4. The cholesterol in our bloodstream has little to do with the cholesterol in our artery walls (i.e., atherosclerosis).
5. The only way sterols end up in artery walls – the one place we don’t want them to be – is if the sterols are carried there by an apoB-containing lipoprotein particle.
6. Inflammation makes it worse, but the inciting event is the LDL particle getting past the endothelium.
7. LDL particles (LDL-P), not LDL cholesterol content (LDL-C), is what drives sterols into artery walls – Don’t confuse the “boats” and the “cargo”.
8. People with metabolic syndrome are at even greater risk of LDL-C/LDL-P discordance.
9. A smaller LDL particle is no more or less atherogenic than a large one – a particle is a particle.
10. The greatest way to reduce your risk of atherosclerosis is to make sure your boats are carrying the right cargo – that way you’ll need fewer of them.
Chris Masterjohn’s overview of cholesterol and heart disease:
(my synopsis of an interview on the podcast Dr. Lo Radio, titled The Truth About Cholesterol With Chris Masterjohn, check out more from Dr. Masterjohn at The Daily Lipid)
Cholesterol
The brain is 2% of the body’s weight but uses 25% of the body’s cholesterol.
Cholesterol is the limiting factor for synapse formation (the connection between brain cells).
When animals (including humans) sleep, the brain makes more cholesterol.
Cholesterol is necessary to make bile acids, which is key in digesting fat and fat soluble vitamins.
Cholesterol is vital for the immune system, having cholesterol in our blood helps protect against pathogens.
Cholesterol is vital to give cell membranes proper fluidity and communication between cells.
Cholesterol is the mother of all steroid hormones. Sex hormones, stress hormones, hormones that regulate blood pressure, mineral balance.
Good and Bad Cholesterol
There is only one kind of cholesterol.
There are different transporters for cholesterol (HDL, LDL, VLDL, etc.).
The common belief supports the Reverse Cholesterol Transport Theory (LDL carries cholesterol into blood and into plaques, HDL gets it out of the blood and back to the liver). Problem- this is not accurate as HDL passes cholesterol to LDL before it gets to the liver. Drugs that prevented this passing of cholesterol ended up killing people. New drugs are currently being tested.
There is a correlation between total cholesterol to HDL and health but it is a correlation.
LDL takes cholesterol to the body allowing it to be utilized.
If LDL isn’t going where it needs to go that’s a problem. You don’t get the nutrients and the LDL particle spends too long in the blood stream and eventually gets oxidated.
When things aren’t used, they go bad.
The key really lies in LDL receptor activity. Receptor activity is governed by two things: native population of cholesterol in the cell (cells low in cholesterol will express more LDL reception) and thyroid hormone (higher levels of thyroid encourage abundance and increased reception).
We want good communication between thyroid and cells.
Low thyroid function could be a reason LDL cholesterol is “high”.
Insulin resistance is also a factor- if insulin can’t communicate well, thyroid conversion from T4 to T3 is hindered, leaving thyroid hampered and impacting cholesterol levels.
Cholesterol Testing
Can be quite useful because it is cheap and widely available.
Don’t get caught up in cause and effect.
Out of range or sudden changes can signify a problem developing.
Thyroid issues can be noted by high cholesterol.
Cholesterol elevated? Think about thyroid function.
Populations free of heart disease: cholesterol 180-220 men, 200-250 women.
If high, look at other markers. Dig deeper. Particularly if total/HDL ratio is low.
Often testosterone is low with these people because thyroid function is low and cells are slowing production.
VAP testing (particle size) is not standardized yet. No strong evidence on which test to use.
The idea of small dense being problematic is correlative and has not been verified via prospective studies. It may just be redundant information. We aren’t sure yet.
Oxidized cholesterol testing is new to the scene, may be good but will take some time to figure out how useful it might be.
Heart Disease
Cholesterol Warriors vs. Cholesterol Skeptics. It’s likely somewhere between.
Need to move beyond the molecules and look to processes going on the body. It’s not the cholesterol in the body that matters, it’s more about why it is there and is it doing its function.
Old rabbit studies: feed cholesterol, they get heart disease. Inject cholesterol into the blood, no heart disease. Inject lipoproteins (e.g. LDL) into blood, heart disease ensued.
Cholesterol doesn’t by itself cause heart disease. Lipoproteins are the problem. Further, the oxidated degeneration of the lipoprotein is the problem. This starts with polyunsaturated fatty acids in particle membrane. But don’t blame them. Blame the process of degeneration.
How do we prevent degeneration? Maintain good thyroid status. Keep good usage and clearance of lipoproteins. Prevent excessive oxidant production by avoiding chronic inflammation and environmental toxins, maintaining a robust metabolism and nourishing the antioxidant defense system. This means getting sufficient protein, B vitamins, selenium, iron, copper, zinc, manganese. How to do that? Eat a nutrient dense diet from both plant and animal origin.
3 key things remain: maintain metabolism, limit oxidants and eat a nourishing diet.
Dr. Thomas Dayspring on cholesterol:
(synopsis of an interview on the podcast The Livin’ La Vida Low Carb Show #585, titled Lipidologist Dr. Thomas Dayspring Explains The Truth About Cholesterol)
Check out more from Dr. Dayspring at LecturePad.org
Lipidology
Science has radically changed, old things we knew as “truth” are almost dead wrong now.
Elevation and research of blood lipids is a rapidly changing field.
Technology to measure cholesterol was there several decades ago so that’s what we studied.
Framingham study showed some correlation so we chased cholesterol as the suspect.
It did seem to follow that cholesterol reduction or LDL cholesterol reduction helped a bit.
Now we get a 30 percent reduction in Arterial Disease (AD) by lowering cholesterol levels. But why don’t the other 70 percent respond?
The reason statins are prescribed is to prevent or reduce atherosclerosis.
If you get a plaque, full of sterols, it will grow and obstruct artery or get inflamed, rupture and then a clot blocks artery.
Sterols in artery wall is the problem. They don’t belong there. Can’t have AD without sterols in the artery wall.
Does cholesterol in blood stream mean anything for cholesterol in artery wall? Maybe some truth but a million exceptions. Tim Russert, LDL of 60 (“ideal” cholesterol), died of a heart attack.
Lipoproteins
Illegal dumpers of cholesterol in artery walls are lipoproteins.
Cholesterol is only trafficked in lipoproteins. Apo-liprotein.
Lipids go nowhere in the human body without a lipoprotein.
Cholesterol can only get into the artery wall if a lipoprotein carries it in there.
Lipoprotein only takes cholesterol where it’s supposed to go.
Atherogenic lipoproteins are the issue, not how much cholesterol they carry.
These particles are the illegal dumpers.
Think about “How many dump trucks?” Not, “how much trash are the trucks carrying?”
We assumed high cholesterol equals high particle count. Almost no norm for this though.
Manage lipoproteins (amount of dump trucks).
Discordant variables are the problem. Example: lots of dump trucks (high LDL particle count with very little trash (low LDL cholesterol). The highest risk is in those where particle count and cholesterol levels don’t match.
Statins up regulate a protein in the liver that grabs the atherogenic particles and pulls them back into the liver. This is good. But did it grab enough of them? If it does the statin helps people. If it doesn’t then they are still at risk. Need to figure this out by looking at particle number.
Lipid Profile
Measures cholesterol trafficked by all lipoproteins in the body.
VLDL comes out of the liver- mostly full of triglycerides but also some cholesterol. As it delivers its triglycerides to cells in the body it shrinks and becomes an LDL. Floats around for a few days and the liver clears it. It is mostly a waste product of a VLDL. LDL is mostly carrying cholesterol.
Cholesterol number is how much cholesterol in one deciliter (3 1/2 oz) of blood.
LDL is simply one of these numbers.
Particle count matters.
NMR LipoProfile is the newest way to get a good look at particle count.
LDL-C: cholesterol count in LDLs.
LDL-P: particle count of LDLs.
Same for HDL.
Protein that wraps every VLDL and LDL- apoliprotein B. One apoB for every VLDL and LDL, a secondary way to count particle number is to see the apoB count is.
VLDL come and go 2-6 hours, LDL is around 2-3 days.
HDL floats around for about 5 days.
Therefore 95% of apoB is LDL related.
High LDL and high particle count/apoB = trouble.
High LDL and normal or low particle count/apoB = low risk.
Low LDL and high particle count/apoB = big risk.
VAP test is interesting but doesn’t really help for health management. That gives a calculated apoB. Need a protein immuno assay of apoB.
Berkeley test does give apoB.
If particle count is high, doesn’t matter what size particles are.
Insulin resistant people have small dense LDL so it has gotten associated with being bad. It is not quite that simple.
Deadliest condition is familial hypercholesterolemia. Homozygous cholesterol in 1000s, die by adolescence. Heterozygotes (300-500) without treatment die of heart attacks in 50s and 60s. They have large fluffy particles. Diabetics who have small dense particles have heart attacks in 50s and 60s.
Lifestyle and diet changes (sometimes medication) are needed to lower risk.
Treatment differs based on risk.
First line treatment is always nutrition. If very high risk add medication.
High particle count? You have too many LDLs because the liver made too many VLDLs. This happens because it has too much fat in it- triglycerides. If you have fat in your liver it will overproduce VLDLs (and make them big) to get rid of them. Triglyceride levels go up. What causes build up of triglycerides? Excess carbohydrates, particularly fructose and HFCS. Culprit is not dietary fat (Unless it is excessive?).
Too many VLDLs = too many LDL.
The LDL ends up carrying fat, which it shouldn’t have that much of. As a result, each LDL has less cholesterol. Blood test looks fine but its not. Normal LDL cholesterol but lots of particles needed to carry the cholesterol.
Get your carbs under control.
No chance of restricting particle count if you keep the carbs high.
Carbs in our insulin resistant world drive the problem (apoB and LDL particle levels) but also raise triglycerides which cause our particles (which should be carrying mostly cholesterol) to become a split carrier of fat and cholesterol.
Triglycerides are a hidden clue. Should be under 70, not 100 (the standard).
Divide triglycerides by HDL. Should be 1. Greater than 3.0 = high particle count and triglyceride rich LDL.
In men, this is the single best lipid predictor of the first heart attack.
Serious marker of insulin resistance and type 2 diabetes.
In women, predicts cardiovascular mortality and all cause mortality.
Saturated fat intake helps improve HDL.
HDL world is changing. HDL shouldn’t be a goal of therapy.
HDL is a small lipoprotein, 95% cholesterol 5% triglycerides
Tons of proteins on outside.
HDL level tells us how much cholesterol your HDL particles have.
VLDL leaves the liver, starts dropping off TGs.
Bumps into LDL and HDL particles along the way.
Lipid transfer protein CEPT, that pulls the TGs out of VLDL and trades TGs for cholesterol.
This is why when TGs go up, people’s HDL C goes down- it’s getting transferred into VLDL.
Same thing happens with LDL.
Low carb diet- very little TGs in the VLDL, very little transfer with LDL and HDL and the cholesterol levels go up.
If HDL gives up too much cholesterol they explode and kidney excretes them.
HDL story is very similar. HDL particle count matters.
HDL-C doesn’t matter if particles are low.
How? Big HDL particles.
Pay less attention to cholesterol and more to particle number.
Less TGs equal more cholesterol in HDL, meaning they have longer shelf life and likely more helping.
Low HDL is usually a risk factor because it means insulin resistance- excessive TGs are causing low HDL C and P.
Low HDL from other factors (genetic) almost no risk for heart disease.
Graveyard is full of high HDL C, low HDL P and high LDL P.
Therapy doesn’t matter if it lowers apoB and LDL P and raises HDL P.
80% of heart disease has insulin resistance as the underlying metabolic disregulation.
Study of 136000 people with a heart attack: 55% had an LDL under 100, 15%’under 70.
Average TGs in US: 140-150.
Look at TGs, HDL/TG ratio and apoB and LDL P.
Finally, Ray Peat gets deep in his article Cholesterol, longevity, intelligence and health. This is a long but good read if you’re interested in cholesterol and what function it might truly have in the body.
Part 3: Questions That Need Answering
Despite all of the advances in cholesterol knowledge, there remains many unanswered questions which are vitally important to both consider and solve.
Here is the big unanswered question:
WHY would your cholesterol end up in your artery walls?
This question opens up an endless array of questions that researchers, doctors, health practitioners and everyone in between is trying to get at…
Is it as random as LDLs crashing into your artery walls?
Or small LDLs getting caught in the cracks of the artery walls?
Where did the cracks come from?
Could your body putting cholesterol there to repair the cracks?
What if you have lots of cholesterol but smooth walls? Then does it matter what size they are or how much cholesterol is in your LDLs?
What if you have tons of cracks but not much cholesterol? Hmmm, this sounds like a heart attack despite low cholesterol numbers…
Is sugar the main culprit of cracks or is it simply stress in any form?
Is it simply a numbers game?
Do you have too many LDL particles and therefore there’s just a higher chance some of them (regardless of the size) get stuck?
But why do you have so many?
Body making them to patch lots of cracks?
Liver not recycling the LDLs?
Too many triglycerides (also housed in LDLs) from a bad diet?
Why so many triglycerides?
LDL receptors on your cells not taking them up?
Could thyroid problems be causing that down regulation?
Are LDLs bad if they don’t get oxidized?
And on and on and on…
Then a whole other line of questions emerge…
What about HDL and its role in all of this?
Have we made the same mistakes in glorifying HDL?
Is there more to the HDL picture?
Ok- enough of that- my head (and likely yours is spinning).
The Bare 5 Bottom Line on Cholesterol:
1. It is vital for life and function.
2. Cholesterol blood levels mean nothing in regard to levels in your artery.
3. We need to consider both LDL and HDL particle count along with cholesterol levels and the quality of the blood and the lipoprotein composition.
4. Use blood tests as clues to the body’s adaptation to your lifestyle.
5. Cholesterol changes happen for a reason, look deeper into what’s going on in the body.
Thanks for reading, have a great week!
P.S. This is what emailed to a client a couple years ago that is still a pretty good summary on how to approach cholesterol…
Just for fun, do an Internet search for Cholesterol myth/lie/scam and just see how much pops up.
Then search for statin side effects and see what pops up.
Here’s a few things to check out:
He’s a functional doctor and therefore has been called a “quack” but he keeps up on current health research better than just about anyone I’ve come across…
http://articles.mercola.com/sites/articles/archive/2010/07/20/the-truth-about-statin-drugs-revealed.aspx
A couple quick you tube videos…
http://m.youtube.com/index?desktop_uri=%2F&gl=US#/watch?v=i8SSCNaaDcE
He’s intense but he knows his stuff…
http://m.youtube.com/index?desktop_uri=%2F&gl=US#/watch?v=OIDoB-CaxP0
http://m.youtube.com/index?desktop_uri=%2F&gl=US#/watch?v=peOaCm4sWgs
There are dozens more doctors writing books like this…
http://www.prweb.com/releases/2011/5/prweb8398286.htm
One of the most thorough and up to date websites on cholesterol…
http://www.cholesterol-and-health.com/
I can also direct you to several podcasts that address cholesterol as well.
Keep in mind that I have the passion and have had the time to keep up with a lot of the forward thinking in the cholesterol research. As an example the thinking has evolved a lot even since some of it was put on the Internet a just few years ago. As an example, if your doctor uses “bad” and “good” cholesterol they probably don’t fully understand the biological role of cholesterol carrying lipoproteins. If they don’t look at ratios of hdl/total or ldl particle count or ApoB or triglycerides or glucose or insulin or markers of inflammation like CRP or (and on and on) then they are a little behind the curve. Not his fault, it’s tough to keep up with.
